Main Text
1 Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive pulmonary disease resulting from inhalation of toxic particulate matter, and is pathologically manifested by pulmonary inflammatory infiltration, airway airflow restriction, bronchial mucosal epithelial lesions, etc. [1-3]. With the progression of COPD, patients may develop respiratory failure and other common complications like pulmonary hypertension (PH), and the combination of COPD and PH can result in the decrease of oxygen uptake in the lungs and increase the risk of death, posing a great threat to the life of patients [4,5]. Relevant research indicated that early screening and treatment of PH has positive effects on improving the prognosis of COPD patients [6]. Right heart cardiac catheterization is a universal clinical method for detecting the presence of PH in COPD patients, but is invasive and has limitations [7]; therefore, finding new serum indicators may be helpful to assist clinical early diagnosis.
The occurrence of COPD complicated with PH is closely associated with inflammation. C-reactive protein (CRP) and albumin (Alb) are both factors related to inflammation, and are often used clinically to evaluate the body’s inflammatory response, the CRP to Alb ratio (CAR) of which is considered a more reliable risk indicator for inflammatory diseases [8]. It has been reported that CAR is strongly correlated with mortality in patients with COPD and CAR could be served as a prognostic biomarker for patients with COPD [9]. Interleukin-28A (IL-28A) belongs to IL-10 family and can participate in regulating the inflammatory response process [10]. Relevant studies have shown that IL-28A is closely related to respiratory virus infectious diseases such as coronavirus pneumonia, and may mediate the occurrence of such diseases clinically, the level of which can be used to assess the severity of the disease [11-13]. C-C motif chemokine ligand 28 (CCL28) is a type of mucosal associated chemokine, and its expression level increases in mucosal epithelium such as the trachea in response to an increase in pro-inflammatory factors [14,15]. Moreover, the level of IL-28A and CCL28 in serum of COPD patients with PH were significantly higher than those in COPD patients without PH [16]. It suggests that these factors may be biomarkers for the diagnosis of COPD combined with PH.
Herein, this study investigated the differences in serum factor levels between COPD patients complicated with or without PH and its predictive value in COPD patients complicated with PH.
2 Materials and methods
2.1 General information
A total of 110 patients with COPD treated in our hospital from January 2021 to February 2023 were included. Based on whether they had combined PH, they were divided into COPD combined with PH group (COPD-PH group, n = 54) and COPD combined without PH group (non-COPD PH group, n = 56). The diagnostic of PH meets the diagnostic criteria in the "Chinese guidelines for the diagnosis and treatment of pulmonary hypertension 2018" [17]. This study approved by the Ethics Committee of our hospital, and it was conducted in accordance with the Declaration of Helsinkiand Ethical Statement. There were no statistically significant differences in terms of gender, age, body mass index (BMI) and smoking status (p > 0.05, Table 1).
Table 1 Comparison of general information between the two groups.
| Group | COPD-PH group (n = 54) | Non-COPD-PH group (n = 56) | X2/t | p | |
|---|---|---|---|---|---|
| Gender (case) | Male | 30 | 23 | 2.310 | 0.129 |
| Female | 24 | 33 | |||
| Age (years) | 45.69 ± 3.12 | 44.87 ± 3.50 | 1.295 | 0.198 | |
| BMI (kg/m2) | 24.85 ± 2.47 | 24.43 ± 2.68 | 0.854 | 0.395 | |
| Smoking (case) | Yes | 28 | 31 | 0.136 | 0.712 |
| No | 26 | 25 | |||
2.2 Inclusion and exclusion criteria
2.2.1 Inclusion criteria
(1) The diagnostic of COPD meets the diagnostic criteria in the "Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021)" [18]; (2) Complete clinical data and signed informed consent.
2.2.2 Exclusion criteria
(1) Heart related diseases such as heart failure; (2) Other lung related diseases such as lung cancer and pulmonary artery stenosis; (3) Long term hypertension; (4) Malignant tumors; (5) Metabolic, immune, and coagulation dysfunction; (6) Abnormal liver and kidney functions; (7) Pregnant and lactating women; (8) Mental illness and poor compliance.
2.3 Research indicators
On the morning of the day after admission, 5 mL fasting peripheral venous blood was collected from two groups of patients, placed in dry sterile test tubes, and centrifuged at 3000 r/min for 10 min to separate serum for laboratory testing.
2.3.1 Clinical indicator level
The clinical indicators of two groups of patients were collected and analyzed, including white blood cell (WBC) count, partial pressure of oxygen (PaO2), arterial partial pressure of carbon dioxide (PaCO2), and forced expiratory volume in one second/forced vital capacity (FEV1/FVC). A fully automated biochemical analyzer (OTA-400, Shenyang Wantai Medical Equipment Co., Ltd., China) was applied to detect WBC count using turbidimetry. A blood gas analyzer (Kangli BG-800A, Meizhou Kangli High tech Co., Ltd., China) was employed to measure PaO2 and PaCO2. A lung function analyzer (BK-LFT-I, Shandong Gaoxin Biosensor Research Institute Co., Ltd.) was exploited to detect and record FEV1 and FVC, and calculate FEV1/FVC ratio.
2.3.2 Serum cytokines
Enzyme-linked immunosorbent assay (ELISA) was carried to detect the levels of CRP, Alb, CCL28, and IL-28A, and CAR was calculated using reagent kit as per the instructions.
2.4 Statistical methods
Statistical analysis was conducted using SPSS 20.0. The count data were represented as n and compared using a X2 test. The Kolmogorov-Smirnov method was used to perform normality analysis on the measurement data. Continuous variables that followed a normal distribution were described as mean ± standard deviation, and independent sample t-test was used for comparison between the two groups. The diagnostic value of each parameter was analyzed using the area under curve (AUC) of the receiver operating characteristic (ROC) and and binary logistic regression analysis. A difference of bilateral p < 0.05 was considered statistically significant.
3 Results
3.1 Comparison of clinical indicators between the two groups of patients
The WBC, PaO2, PaCO2 and FEV1/FVC ratio displayed no significantly statistical difference between the two groups of patients (p > 0.05, Table 2).
Table 2 Comparison of clinical indicators between the two groups of patients (mean ± standard deviation).
| Group | Case | WBC (109/L) | PaO2 (mmHg) | PaCO2 (mmHg) | FEV1/FVC (%) |
|---|---|---|---|---|---|
| COPD-PH group | 54 | 9.85 ± 7.23 | 72.58 ± 4.12 | 41.03 ± 13.24 | 53.45 ± 8.74 |
| Non-COPD-PH group | 56 | 11.64 ± 8.82 | 73.38 ± 4.96 | 42.66 ± 15.89 | 52.13 ± 9.48 |
| t | -1.162 | -0.918 | -0.583 | 0.759 | |
| p | 0.248 | 0.360 | 0.561 | 0.450 |
3.2 Comparison of CAR, IL-28A and CCL28 levels between the two groups of patients
The CRP, Alb, CAR, IL-28A and CCL28 levels were higher in COPD-PH group than non-COPD-PH group (p < 0.05, Table 3).
Table 3 Comparison of CAR, IL-28A and CCL28 levels between the two groups of patients (mean ± standard deviation).
| Observation indicators | COPD-PH group (n = 54) | Non-COPD-PH group (n = 56) | t | p |
|---|---|---|---|---|
| CRP (mg/L) | 25.28 ± 6.33 | 4.35 ± 2.62 | 22.804 | 0.000 |
| Alb (g/L) | 41.25 ± 8.29 | 36.42 ± 4.30 | 3.856 | 0.000 |
| CAR | 1.30 ± 0.52 | 0.30 ± 0.27 | 12.723 | 0.000 |
| IL-28A (pg/mL) | 411.63 ± 75.28 | 241.82 ± 61.93 | 12.940 | 0.000 |
| CCL28 (pg/mL) | 3.31 ± 0.72 | 1.34 ± 0.72 | 14.346 | 0.000 |
3.3 Multivariate logistic analysis of COPD combined with PH
Logistic regression analysis showed that CAR, IL-28A, and CCL28 are all risk factors for COPD complicated with PH (Table 4).
Table 4 Multivariate logistic analysis of COPD combined with PH.
| Influencing factors | β | SE | Wald X2 | p | OR | 95% CI |
|---|---|---|---|---|---|---|
| CAR | 2.334 | 0.898 | 6.755 | 0.009 | 10.324 | 1.775 - 60.029 |
| IL-28A | 0.012 | 0.006 | 4.108 | 0.043 | 1.012 | 1.000 - 1.024 |
| CCL28 | 1.167 | 0.513 | 5.172 | 0.023 | 3.212 | 1.175 - 8.779 |
3.4 The predicative value of CAR, IL-28A and CCL28 levels for COPD combined with PH
The AUC values of serum CAR, IL-28A, CCL28 and their combination on COPD combined with PH were 0.930, 0.948, 0.957 and 0.973, respectively (p < 0.05, Table 5 and Figure 1).
Table 5 The predicative value of CAR, IL-28A and CCL28 levels for COPD combined with PH.
| Indicators | AUC | 95% CI | Sensitivity | Specificity |
|---|---|---|---|---|
| CAR | 0.930 | 0.876 - 0.984 | 0.871 | 0.964 |
| IL-28A | 0.948 | 0.899 - 0.998 | 0.908 | 0.982 |
| CCL28 | 0.957 | 0.913 - 1.000 | 0.890 | 0.946 |
| Combined prediction | 0.973 | 0.937 - 1.000 | 0.927 | 0.964 |
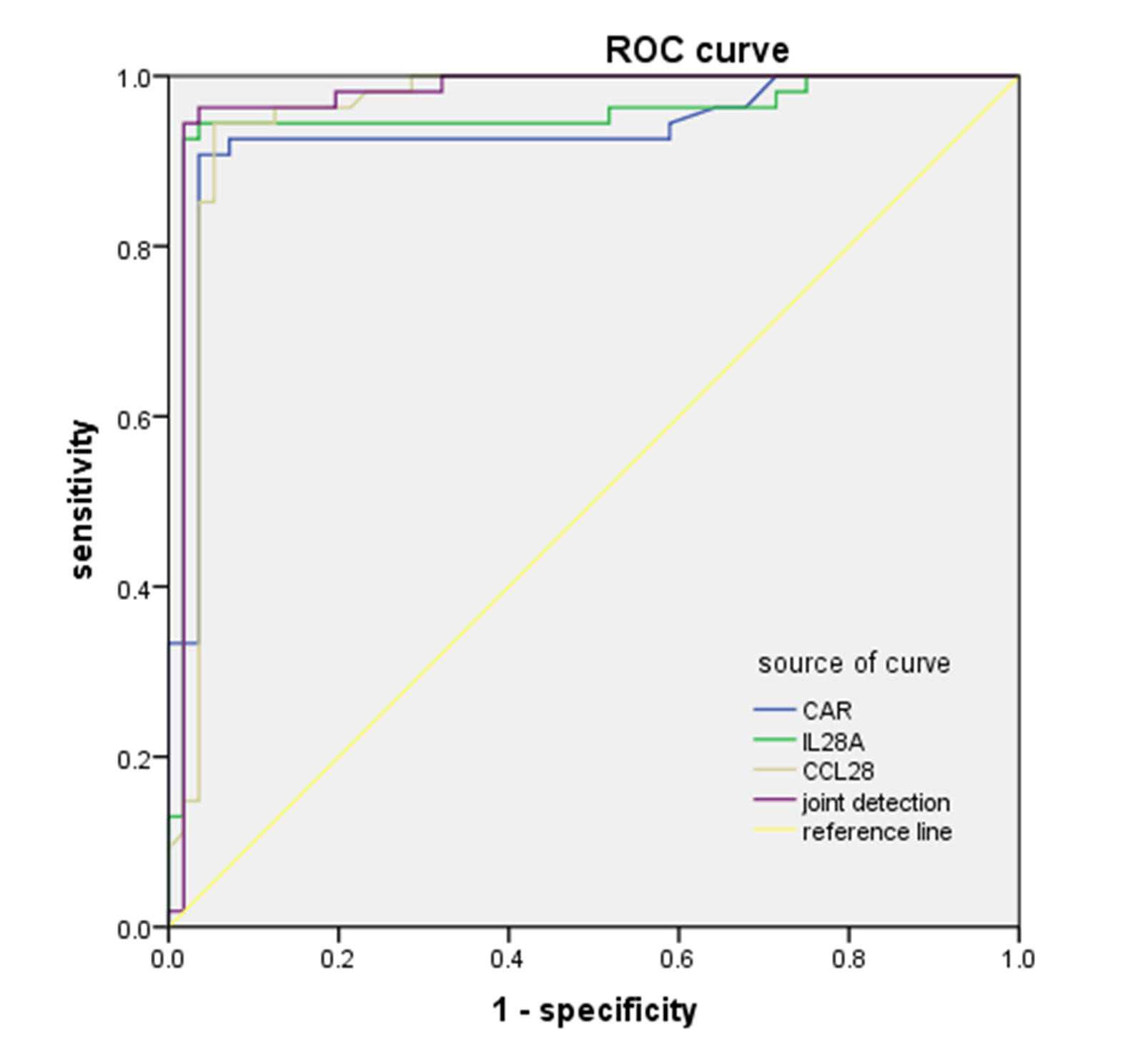
Figure 1 The ROC curve of CAR, IL-28A and CCL28 levels for COPD combined with PH.
4 Discussion
To find effective prediction indicators for COPD patients combined with PH, this study statistically collected and compared clinical data and serum factors such as CAR, IL-28A, CCL28, etc. between COPD patients with and without PH, dissected the risk factors of PH in COPD patients, and evaluated the predictive value of CAR, IL-28A and CCL28 using ROC curve. The results indicated that CAR, IL-28A and CCL28 in combination had relatively higher predictive value for the occurrence of PH in COPD patients.
Our results found no obvious difference in WBC, PaO2, PaCO2 and FEV1/FVC level between COPD-PH and non-COPD-PH groups, but CRP, Alb, CAR, IL-28A and CCL28 levels were higher in COPD-PH group than non-COPD-PH group, hinting that inflammation levels were relatively high in COPD patients combined with PH, and the CRP, Alb, CAR, IL-28A and CCL28 may mediate the occurrence of PH. CAR refers to the ratio of CRP and Alb, of which CRP is a kind of inflammatory proteins with a high level indicating aggravated inflammation and infection, while Alb is a kind of protein possessing multiple physiological functions (regulating inflammatory responses and maintaining plasma prosthesis osmotic pressure), with a low level indicating inflammation [9]. The elevated levels of CRP and Alb in the lungs of COPD patients can cause endothelial dysfunction and vascular remodeling in the lungs, and meanwhile also increase the resistance of blood and gas circulation in the lungs, leading to the development of PH in COPD patients [19]. IL-28A, also known as interferon λ3, can bind to IL-28A receptors to form complexes and mediate signaling pathways such as tyrosine kinases, enhancing interferon stimulated gene expression and exerting anti-infective effects [20]. IL-28A up-regulation denotes the aggravation of infection in COPD patients, and also exacerbates pulmonary vascular endothelial injury, increasing the risk of PH. It has been reported that IL-28A may up-regulate inflammatory cytokines to induce COPD combined with PH and exhibits a higher level in COPD patients combined with PH compared to COPD patients [21], consistent with our results. CCL28 is mainly distributed in the mucosal tissues, and its C-terminus carries positively charged amino acid pairs. At the same time, CCL28 can also regulate the secretion of immune cells such as immunoglobulin A, and therefore participate in regulating the inflammatory response process [22]. The binding between CCL28 and receptors can recruit immune cells to inflammatory parts, aggravate inflammation response, further damage epithelial tissues in the lung and promote the occurrence of PH [23]. Besides, serum CCL28 level has been confirmed to be elevated in COPD patients combined with PH relative to COPD patients [24], consistent with our findings.
Based on the above results, this study proved that CAR, IL-28A and CCL28 may participate in the progression of COPD and induce PH. Therefore, this study used logistic multiple regression analysis to identify the risk factors for PH in COPD patients. The results suggested that CAR, IL-28A, and CCL28 were all risk factors for PH occurrence. In addition, a study on the serum cytokine profile of COPD related PH patients showed that there were differences in the levels of serum IL-28A and CCL28 between COPD patients with PH and COPD patients, implying that IL-28A and CCL28 may serve as biomarkers for the diagnosis and prognosis COPD complicated with PH [16]. Similar results were obtained in this study. Moreover, the existing report revealed that CAR may predict the progression of respiratory system diseases in patients [16,25]. Hence, this study further assessed the predictive value of CAR, IL-28A and CCL28 on COPD complicated with PH using ROC curve and confirmed that the combined prediction had the highest AUC value, manifesting that CAR, IL-28A and CCL28 in combination had a relatively high predictive value against PH occurrence. During the clinical prediction of COPD patients, when the above factors showed abnormal levels, necessary measures should be taken to prevent the occurrence of PH.
In conclusion, serum CAR, IL-28A and CCL28 has predictive value towards COPD combined with PH, and can be used to assist PH screening in COPD patients. Owing to the limited sample size and in order to reduce the impact of accidental bias on research results, future research requires more sample size to further verify the predictive value of CAR, IL-28A and CCL28 on COPD combined with PH. More prospective studies are needed in the future to confirm this result with more patients and long-term follow-up.
Back Matter
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Conceptualization, Writing – original draft, X.K.; Data curation, Writing – review and editing H.Z. All authors have read and agreed to the published version of manuscript.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee, and patients were informed and consented.
Funding
Not applicable.
Availability of Data and Materials
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Supplementary Materials
Not applicable.
References
- Kaur M, Chandel J, Malik J, et al. Particulate matter in COPD pathogenesis: an overview. Inflammation research 2022; 71(7-8): 797-815.
- Christenson SA, Smith BM, Bafadhel M, et al. Chronic obstructive pulmonary disease. Lancet 2022; 399(10342): 2227-2242.
- Guo P, Li R, Piao TH, et al. Pathological Mechanism and Targeted Drugs of COPD. International Journal of Chronic Obstructive Pulmonary Disease 2022; 17: 1565-1575.
- Ferri S, Paoletti G, Pelaia C, et al. COPD and biologic treatment: state of the art. Current Opinion in Allergy and Clinical Immunology 2023; 23(4): 309-318.
- Olsson KM, Corte TJ, Kamp JC, et al. Pulmonary hypertension associated with lung disease: new insights into pathomechanisms, diagnosis, and management. The Lancet. Respiratory Medicine 2023; 11(9): 820-835.
- Singhvi D, Bon J. CT Imaging and Comorbidities in COPD: Beyond Lung Cancer Screening. Chest 2021; 159(1): 147-153.
- Kovacs G, Avian A, Bachmaier G, et al. Severe Pulmonary Hypertension in COPD: Impact on Survival and Diagnostic Approach. Chest 2022; 162(1): 202-212.
- Kunutsor SK, Laukkanen JA. Serum C-reactive protein-to-albumin ratio is a potential risk indicator for pneumonia: Findings from a prospective cohort study. Respiratory medicine 2022; 199: 106894.
- Shen S, Xiao Y. Association Between C-Reactive Protein and Albumin Ratios and Risk of Mortality in Patients with Chronic Obstructive Pulmonary Disease. International Journal of Chronic Obstructive Pulmonary Disease 2023; 18: 2289-2303.
- Xu S, Zhang J, Liu J, et al. The role of interleukin-10 family members in cardiovascular diseases. International Immunopharmacology 2021; 94: 107475.
- Shokri M, Khonakdar OG, Mohammadnia-Afrouzi M, et al. Posttreatment Downregulation of Type III Interferons in Patients with Acute Brucellosis. Mediators of Inflammation 2021; 2021: 8601614.
- Fukuda Y, Homma T, Inoue H, et al. Serum IL-28A/IFN-λ2 is linked to disease severity of COVID-19. Scientific Reports 2022; 12(1): 5458.
- Fukuda Y, Homma T, Inoue H, et al. Downregulation of type III interferons in patients with severe COVID-19. Journal of Medical Virology 2021; 93(7): 4559-4563.
- Dhanushkodi NR, Prakash S, Quadiri A, et al. Mucosal CCL28 Chemokine Improves Protection against Genital Herpes through Mobilization of Antiviral Effector Memory CCR10+CD44+ CD62L-CD8+ T Cells and Memory CCR10+B220+CD27+ B Cells into the Infected Vaginal Mucosa. Journal of Immunology 2023; 211(1): 118-129.
- Chen F, Yang SY, Fang XX, et al. Role of the CCL28-CCR10 pathway in monocyte migration in rheumatoid arthritis. Journal of Peking University (Health Sciences) 2022; 54(6): 1074-1078.
- Zhang Y, Lin P, Hong C, et al. Serum cytokine profiles in patients with chronic obstructive pulmonary disease associated pulmonary hypertension identified using protein array. Cytokine 2018; 111: 342-349.
- Working Group on Pulmonary Vascular Diseases of Chinese Society of Cardiology of Chinese Medical Association; Editorial Board of Chinese Journal of Cardiology. Chinese guidelines for the diagnosis and treatment of pulmonary hypertension 2018. Zhonghua Xin Xue Guan Bing Za Zhi 2018; 46(12): 933-964.
- Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society; Chronic Obstructive Pulmonary Disease Committee of Chinese Association of Chest Physician. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (revised version 2021). Zhonghua Jie He He Hu Xi Za Zhi 2021; 44(3): 170-205.
- Xu MY, Han XP, Liu YL, et al. Risk factors of pulmonary hypertension in acute exacerbation of chronic obstructive pulmonary disease. The Journal of Practical Medicine 2022; 38(19): 2467-2471.
- Zhu HZ, Butera M, Nelson DR, et al. Novel type I interferon IL-28A suppresses hepatitis C viral RNA replication. Virology Journal 2005; 2: 80.
- Sun Y, Qiu HB, Ge HT, et al. Expression and Clinical Significance of Serum AgRP and IL-28A in Chronic Obstructive Pulmonary Disease Compli-cated with Pulmonary Hypertension. Clinical Misdiagnosis & Mistherapy 2022; 35(10): 68-73.
- Wilsona E & Butchera EC. CCL28 Controls Immunoglobulin (Ig)A Plasma Cell Accumulation in the Lactating Mammary Gland and IgA Antibody Transfer to the Neonate. The Journal of Experimental Medicine 2004; 200(6): 805–809.
- Yan YF, Wang ZY & Liu J. Study on the expression of CCL 28 in serum of patients with acute asthma attacks. Journal of Molecular Diagnostics and Therapy 2024; 16(5): 975-978+984.
- Sun L, Ma JF & Cui NF. Expression of Serum CCL28 and SDF-1 in Patients with Chronic Obstructive Pulmonary Disease Complicated by Pulmonary Hypertension and Its Clinical Significance. Journal of Modern Laboratory Medicine 2023; 38(1): 140-146.
- Li Y, Li H, Song C, et al. Early Prediction of Disease Progression in Patients with Severe COVID-19 Using C-Reactive Protein to Albumin Ratio. Disease Markers 2021; 2021: 6304189.